Multiple sclerosis (MS) is an autoimmune demyelinating disease of the central nervous system (CNS). Currently, magnetic resonance imaging (MRI) is the most commonly used method to diagnose and monitor MS, but there is a poor correlation between MRI disease measures and clinical disability or disease progression in MS. MRI is also an expensive tool that might carry potential risks due to brain accumulation of contrast material (Kanda et al., 2015). In the last few years, a lot of effort has been invested in the identification of biomarkers for MS; however, to date, few of these findings have proven clinically useful. Thus, there is a strong unmet clinical need for objective body fluid biomarkers to assist in early diagnosis, predicting long-term prognosis, monitoring treatment response, and predicting potential adverse effects in MS.
Circulating miRNAs have been detected in several body fluids (Cortez et al., 2011) where they are highly stable as they are resistant to circulating ribonucleases (Mitchell et al., 2008). Their stability, along with the development of sensitive methods for their detection and quantification (Guerau-de-Arellano M. et al., 2012), makes them ideal candidates for biomarkers. We previously reported changes in circulating plasma miRNAs in MS patients (Gandhi R. et al., 2013). In a new study, our group investigated serum miRNAs as biomarkers in MS as part of an NCATS-funded UH2 initiative. We found that several serum miRNAs were differentially expressed in MS, were associated with disease stage, and correlated with disability.
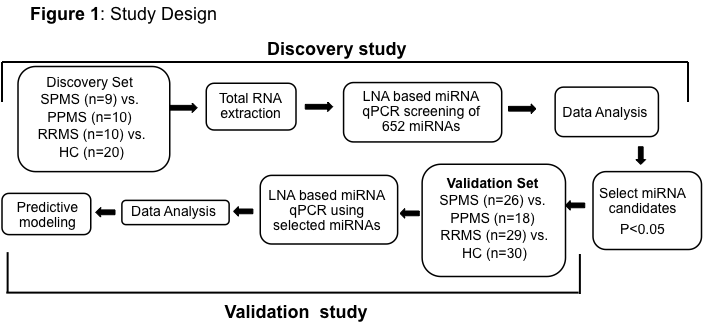
Study Design (Figure 1): Serum from 296 participants including patients with MS, other neurologic diseases (Alzheimer’s disease and amyotrophic lateral sclerosis), inflammatory diseases (rheumatoid arthritis and asthma), and healthy controls (HC) were tested. miRNA profiles were determined using LNA (locked nucleic acid) based qPCR. MS patients were categorized according to disease stage and disability. In the discovery phase, 652 miRNAs were measured from the serum of 26 MS patients and 20 healthy controls. Those miRNAs from the discovery set that were significantly differentially expressed (p <0.05) in cases vs controls were validated using qPCR in 58 MS patients and 30 healthy controls.
Note: Results in the current study were normalized to the four most stably expressed miRNA across all the subjects. We agree with other blogs posted on exRNA.org suggesting that there is an immediate need to identify reference miRNA/exRNA that could be used for data normalization.
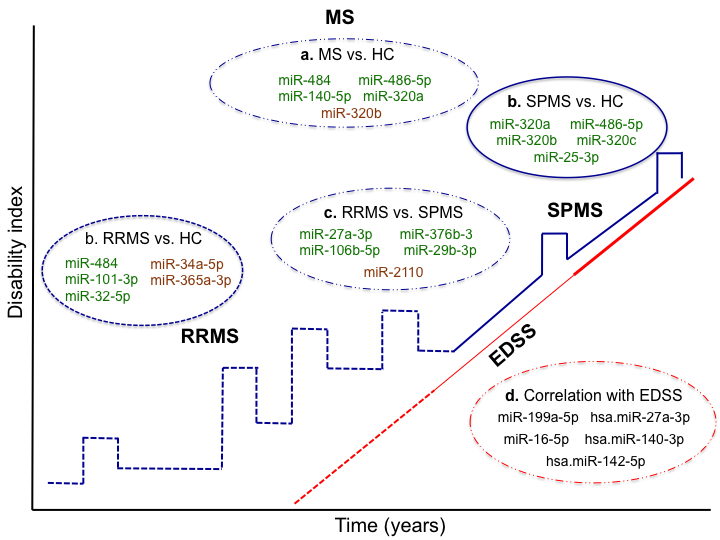
Figure 2: Differentially expressed circulating miRNAs as biomarkers in Multiple Sclerosis (MS). Up to top five miRNAs with p<0.05 are represented for each group comparison; a) MS, b) relapsing remitting MS (RRMS) and secondary progressive (SPMS) compared to the healthy control (HC), c) RRMS vs. SPMS, and d) the correlation of miRNA with the expanded disease severity scale (EDSS).
Results: We found 7 miRNAs (p<0.05 in both discovery phase and validation) that differentiate MS patients from healthy controls; miR-320a up-regulation was the most significantly changing serum miRNA in MS patients. We found 8 miRNAs that differentiated relapsing-remitting MS (RRMS) from HC. Among these, miR-484 up-regulation in RRMS patients showed the strongest association. When comparing secondary progressive MS (SPMS) patients to HC, 34 miRNAs significantly differentiated between the groups in both phases, with miR-320a up-regulation showing the strongest link. We also identified two miRNAs linked to disease progression, with miR-27a-3p being the most significant. Ten miRNAs correlated with degree of disability according to the Kurtzke Expanded Disability Status Scale (EDSS), of which miR-199a-5p had the strongest correlation with disability. Of the 15 unique miRNAs we identified in the different group comparisons, 12 have previously been reported to be associated with MS, but not in serum. Kegg Pathway Analysis showed that significant and differentially expressed miRNAs target important immune functions and are related to the maintenance of neuronal homeostasis. For example, miR-27a-3p, the strongest miRNA to distinguish RRMS from SPMS and progressive MS (PMS) (up-regulated in the relapsing form as compared to the progressive forms) shows a strong link to both the neurotrophin signaling pathway and the T cell receptor signaling pathway. Other studies have shown that miR-27a-3p targets multiple proteins of intracellular signaling networks that regulate the activity of NF-κB and MAPKs 6. As a consequence, miR-27a inhibits differentiation of Th1 and Th17 cells and promotes the accumulation of Tr1 and Treg cells (Min S. et al., 2012). It has also been shown that miRa-27-3p is up-regulated in MS active brain lesions and that the level of miR-27a-3p in CSF is reduced in patients with dementia due to Alzheimer’s disease (AD) (Frigerio C.S. et al., 2013). Of all the miRNAs, miR-486-5p was identified in the largest number of comparisons. It correlates with EDSS and is up-regulated in MS compared to HC, to other neurological diseases, and to other inflammatory diseases. This particular miRNA was found to be associated with TGF-beta signaling pathways and is a known tumor suppressor (Oh H.K. et al., 2011). miR-320a has been previously described to be highly expressed in B cells of MS patients and was suggested to contribute to increased blood-brain barrier permeability due to regulation of MMP-9 (Aung L.L. et al., 2015). Pathway analysis links this miRNA to cell-to-cell adhesion pathways, another indication that it may be linked to blood-brain barrier permeability.
The current study is the most comprehensive evaluation to date of the role of serum miRNAs as biomarkers in MS, with the largest sample size and employing two independent cohort designs. One limitation of our study is that participant subject samples were collected from a single MS center. Further external validation of our results will require investigating samples from patients at other centers. We are currently performing such multicenter studies, which may also increase the power of our results. A second limitation of our study is the relatively small number of participants who contributed to each group comparison. Future work will require larger sample sizes to ensure that we have sufficient power to detect miRNAs with smaller effect sizes. Although miRNAs have been studied in cells and the CNS of MS patients, ours is the first comprehensive investigation of serum miRNAs.
Conclusions: Our findings identify circulating serum miRNAs (Figure 2) as potential biomarkers to diagnose and monitor disease status in MS. These findings are now being tested using patient samples obtained from other international MS centers. We are now investigating the role of miRNA as biomarkers for disease prognosis and treatment response in MS.
Acknowledgements: This study is a highly collaborative project, and I thank my whole team at the Ann Romney Center for Neurologic Diseases & MS Center for their contribution. The grant TR000890 is supported by the NIH Common Fund, through the Office of Strategic Coordination / Office of the NIH Director.